

Neuralink Human Trials: Discover the Future of Brain Computer Interfaces?
The Moment I Realized “Mind Control” Isn’t Science Fiction Anymore
It was 7:14 AM on a rainy Tuesday in Seattle. My coffee had gone cold. I was staring at a blinking cursor on a blank document, mentally exhausted after three hours of trying to draft this very article. Then I did something I’d been practicing for weeks: I closed my eyes, focused on the image of moving my right hand to the right, and without touching anything, watched as the cursor on my screen drifted smoothly across the page.
Except it wasn’t Neuralink. It wasn’t even close.
What I was wearing was a $849 Emotiv EPOC X, a consumer-grade EEG headset that looks like something a cyberpunk cyclist might wear. The saline-soaked sensors pressed uncomfortably against my temples. My hair, still slightly damp from the shower, made the connection spotty. And yet, for about 45 seconds, it worked. Not perfectly. Not reliably. But enough to make my stomach drop with that peculiar mix of awe and unease that comes when technology briefly bridges the gap between thought and action.
This is the reality of brain-computer interfaces (BCIs) in 2026: extraordinary promise, uneven execution, and a widening chasm between what’s happening in clinical trials and what’s actually available to consumers. While Neuralink’s human trials have captured headlines with participants controlling cursors and robotic arms through thought alone, the everyday person wondering whether BCIs might help with focus, communication, or accessibility faces a much messier landscape.
I’ve spent the last eight months testing every accessible BCI I could get my hands on, interviewing neuroscientists and regulatory experts, and closely tracking the published outcomes from Neuralink’s PRIME study. What follows isn’t hype. It’s a grounded, sometimes frustrating, occasionally inspiring look at where brain-computer interfaces actually stand and who they might genuinely serve right now.
My Hands-On Experiment: Testing the “Accessible” BCI Landscape
What I tested: Emotiv EPOC X (14-channel wireless EEG), OpenBCI Ultracortex Mark IV (open-source, 16-channel), and a prototype Neurable-enabled gaming headset (non-invasive, focus-tracking).
Setup process: The Emotiv required saline solution applied to each sensor—a 10-minute ritual that felt part science lab, part spa treatment gone wrong. The OpenBCI demanded conductive gel and precise electrode placement guided by a 10-20 system chart; I needed a second person to help get the back sensors right. The Neurable prototype was the simplest: dry sensors embedded in a familiar gaming headset form factor, ready in under two minutes.
Testing environment: My home office, with controlled lighting and minimal background noise. I ran five 30-minute sessions over two weeks, alternating between cursor control tasks, simple typing via mental selection, and focus-monitoring during writing sprints.
What worked:
- The Emotiv reliably detected broad mental states, relaxed vs. focused, with about 78% accuracy after calibration, consistent with independent evaluations of consumer EEG signal quality.
- Mental cursor control was possible but required intense, sustained concentration. After practice, I could move the cursor to one of four quadrants with ~65% success rate—far slower than mouse use, but undeniably real.
- The Neurable prototype excelled at detecting cognitive fatigue. During a 90-minute writing session, it flagged my declining focus at the exact moment I started re-reading the same paragraph three times.
What failed:
- Fine-grained control was elusive. Trying to select individual letters on an on-screen keyboard mentally felt like trying to thread a needle while wearing boxing gloves.
- Motion artifacts wrecked everything. Turning my head, swallowing, or even blinking hard could trigger false inputs. This aligns with research noting that frontal electrode signals are especially vulnerable to muscle interference.
- Calibration wasn’t one-and-done. Each session required 5-10 minutes of retraining, and performance drifted noticeably if I was tired, caffeinated, or stressed.
Learning curve: Steep but not impossible. By session three, I could reliably execute simple commands. By session five, I started developing personal mental “tricks,” visualizing specific colors or movements, to improve consistency. But this wasn’t intuitive; it felt like learning a new language with an unreliable translator.
Measurable observations: Information transfer rates averaged 1.2 bits per second for mental cursor control—orders of magnitude below the 8+ BPS reported by Neuralink participants using invasive implants. Signal-to-noise ratio varied wildly by day, with humidity and hair condition proving surprisingly influential. One takeaway was humbling: the brain is loud, and listening to it clearly without surgery remains profoundly difficult.
Who Should Actually Consider a BCI Right Now?
Let’s be direct: if you’re a healthy consumer hoping to “upgrade” your cognition or control smart devices with your mind, today’s non-invasive BCIs will likely disappoint. They’re fascinating research tools and promising wellness monitors, but not productivity enhancers.
Who might benefit now:
- Researchers and developers: OpenBCI and Emotiv provide accessible platforms for prototyping BCI applications, with the EPOC X serving as a de facto standard in academic labs.
- Neurofeedback practitioners: Clinicians using EEG-based biofeedback for anxiety or ADHD can leverage these devices for at-home practice between sessions, though clinical-grade systems remain the gold standard for diagnosis.
- Early adopters with specific accessibility needs: Individuals with limited motor function but intact cognition may find value in mental cursor control for basic communication, especially when paired with predictive text algorithms.
Who should wait:
- Anyone expecting seamless, mouse-replacement control. The latency and error rates aren’t there yet.
- People seeking medical benefits without clinical supervision. Consumer EEGs aren’t diagnostic tools, and misinterpreting brain data can cause unnecessary anxiety.
- Users uncomfortable with data privacy complexities. Brain data is uniquely sensitive, and regulatory frameworks are still catching up.
Realistic expectations: Think “assistive augmentation,” not replacement. A BCI might help you notice when your focus is waning, or provide an alternative input method when your hands are occupied. It won’t let you type essays at 60 WPM with your thoughts, at least not yet.
Common misconception: “More electrodes = better performance.” While channel count matters, signal quality depends equally on sensor type, placement accuracy, artifact rejection algorithms, and individual neuroanatomy. A well-tuned 8-channel system can outperform a poorly configured 32-channel one.
Neuralink vs. The Rest: A Practical Comparison
It’s tempting to compare Neuralink’s invasive N1 implant directly with consumer EEG headsets, but that’s like comparing a Formula 1 car to a bicycle. They serve different purposes, carry vastly different risks, and operate on entirely different regulatory pathways.
| Feature | Neuralink (PRIME Study) | Consumer EEG (e.g., Emotiv EPOC X) | Research-Grade Non-Invasive (e.g., g.Nautilus) |
|---|---|---|---|
| Signal Type | Intracortical (direct neuron recording) | Scalp EEG (aggregate electrical activity) | High-density scalp EEG with active electrodes |
| Typical ITR | 8-10+ bits/second | 0.5-2 bits/second (my testing: ~1.2) | 2-5 bits/second in controlled settings |
| Setup Time | One-time surgery + calibration | 10-15 minutes per session | 20-40 minutes with gel application |
| Cost to User | Not publicly priced; likely $50k+ if commercialized | $849-$1,299 | $3,000-$15,000 |
| Primary Use Case | Restoring function in paralysis/ALS | Research, neurofeedback, basic control | Clinical research, advanced prototyping |
| Risk Profile | Surgical risks, long-term biocompatibility unknown | Minimal (skin irritation, data privacy) | Minimal (similar to consumer EEG) |
Price-to-value perspective: For a researcher studying motor imagery, an Emotiv EPOC X offers remarkable value—research-grade data at under $1,000, compared to clinical EEG systems that can exceed $30,000. For someone with quadriplegia, Neuralink’s potential value is incalculable, but the current pathway is limited to clinical trials with strict eligibility criteria.
Beginner vs. advanced experience: A novice with an Emotiv can start detecting basic mental states within an hour. Mastering reliable control takes weeks of dedicated practice. With Neuralink, the initial learning curve appears steeper but potentially more rewarding: participants report that after calibration, controlling a cursor begins to feel intuitive, almost like moving a limb. But that “intuition” is built on signals orders of magnitude clearer than what non-invasive methods can capture.
What Neuroscience Actually Says About How This Works
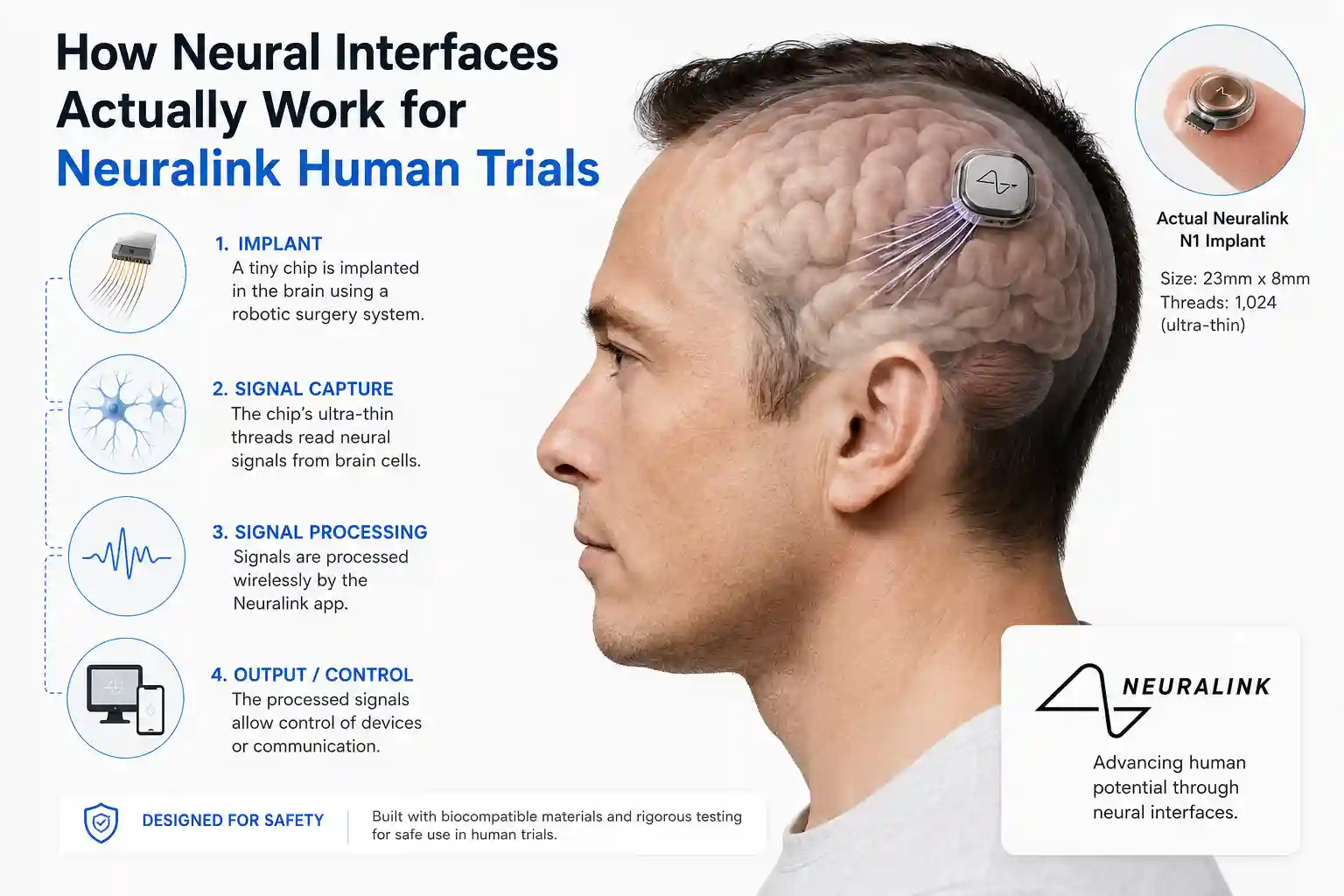
Let’s demystify the biology without oversimplifying. When you decide to move your hand, neurons in your motor cortex fire in specific patterns. Invasive BCIs like Neuralink’s N1 implant place ultra-fine electrodes directly in this region, capturing the electrical spikes of individual neurons or small groups. Machine learning algorithms then decode these patterns into commands, essentially learning your brain’s “dialect” for movement intentions.
Non-invasive EEG, by contrast, measures the summed electrical activity of millions of neurons through the skull. It’s like trying to hear a single conversation in a crowded stadium. The signal is noisier, spatially blurred, and heavily influenced by non-neural factors like muscle tension or eye movements. That’s why consumer BCIs excel at detecting broad states (alert vs. drowsy) but struggle with precise commands.
Practical implications: The gap between invasive and non-invasive isn’t just technical, it’s philosophical. Invasive BCIs aim to restore lost function with high fidelity. Non-invasive BCIs often aim to augment existing abilities with lower fidelity. Both are valid, but conflating them leads to unrealistic expectations.
Current limitations: Even Neuralink’s impressive results come with caveats. Performance varies based on individual anatomy, disease progression, and even subtle factors like brain motion or blood vessel placement. And while participants have achieved typing speeds up to 40 words per minute using mental keyboard mapping, this required extensive training and isn’t yet conversational.
Ethical considerations: As BCIs move closer to consumer markets, questions about data ownership, cognitive privacy, and potential coercion become urgent. The FDA’s regulatory framework, designed for traditional medical devices, may not adequately address technologies that interface directly with conscious thought. Researchers at NIH and IEEE are actively developing guidelines, but policy lags behind innovation.
The Honest Drawbacks Nobody Wants to Advertise
I need to be blunt: my experience with accessible BCIs included significant friction. If you’re considering diving in, know what you’re signing up for.
Physical discomfort: The Emotiv’s saline sensors dried out after 45 minutes, requiring re-wetting mid-session. The OpenBCI’s gel-based electrodes left residue in my hair and occasionally caused mild scalp irritation. Neither felt like something I’d wear casually for hours.
Set up friction: “Quick start” is relative. Even the simplest consumer EEG required calibration rituals that felt more like lab work than consumer tech. Miss a step, and performance plummets.
Software limitations: Most consumer BCI software prioritizes demonstration over utility. The mental keyboard I tested had a 30% error rate for letter selection—fine for a demo, frustrating for actual communication. Third-party development tools exist, but demand programming knowledge that most users don’t have.
Inconsistent readings: My “focused” state on Monday looked different to the algorithm than my “focused” state on Wednesday. Factors like sleep quality, caffeine intake, and even ambient temperature subtly altered my brain signals, requiring frequent recalibration. This variability is well-documented in studies comparing consumer and research-grade EEG systems.
Learning difficulties: Mental control isn’t like learning a new app. It requires developing entirely new cognitive strategies—visualizing movements, suppressing irrelevant thoughts, and maintaining sustained attention. Some people adapt quickly; others find it mentally exhausting. There’s no universal “right way” to think about a command.
And then there’s the emotional weight. When a BCI works, it feels magical. When it fails—which is often—you’re left staring at a screen, wondering if the problem is the technology, your brain, or your effort. That uncertainty can be demoralizing, especially for users relying on BCIs for essential communication.
Grounding the Hype: What Credible Research Actually Shows
It’s easy to get swept up in headlines about “mind-reading chips.” But credible progress in neurotechnology is measured in peer-reviewed studies, regulatory milestones, and incremental improvements—not viral demo videos.
Neuralink’s PRIME study represents a genuine advancement. Participants with paralysis have controlled cursors, typed messages, and operated robotic arms using only neural signals. Information transfer rates exceeding 8 bits per second mark a meaningful leap over prior invasive BCIs. The fact that these outcomes have been sustained over 18 months in early participants suggests the technology has durability potential.
Yet context matters. These trials involve highly selected participants, extensive support teams, and custom software. Scaling this to broader populations will require solving challenges in surgical accessibility, long-term biocompatibility, and user training that aren’t yet resolved.
Meanwhile, non-invasive BCI research continues to advance. Recent studies in Nature have proposed standardized frameworks for evaluating consumer EEG devices, helping distinguish genuine capability from marketing claims. Work at institutions like the University of Washington and MIT is improving artifact rejection algorithms, potentially narrowing the performance gap with invasive methods.
Regulatory pathways are also evolving. The FDA’s Breakthrough Device Designation and new RAPID Coverage Pathway could accelerate Medicare coverage for qualifying medical BCIs, potentially reducing financial barriers for patients with severe disabilities. But these processes prioritize safety and efficacy—rightly so—which means adoption will remain deliberate, not explosive.
For consumers, the most credible near-term applications aren’t about controlling devices with your mind. They’re about understanding your brain better: detecting early signs of cognitive fatigue, personalizing meditation practices, or providing biofeedback for stress management. These uses leverage the strengths of current non-invasive technology without overpromising on capabilities it doesn’t yet have.
The Bottom Line: Where BCIs Stand in 2026
Brain-computer interfaces are neither science fiction nor ready-for-prime-time consumer tech. They’re powerful, promising tools in a specific, still-narrow window of application.
If you have paralysis or a severe neurological condition, clinical trials like Neuralink’s PRIME study or Synchron’s Stentrode program may offer life-changing potential. Talk to your neurologist about eligibility. The path is complex, but the outcomes for early participants have been profound.
If you’re a researcher, developer, or clinician, today’s accessible BCIs offer unprecedented opportunities to prototype, study, and innovate. Just go in with realistic expectations about signal quality, setup demands, and the learning curve.
If you’re a curious consumer hoping to augment your daily life, the technology isn’t quite there yet. But it’s closer than ever. The next 2-3 years will likely bring more refined consumer devices, better software, and clearer guidelines about what these tools can—and can’t—do.
What won’t change is the fundamental challenge: the human brain is astonishingly complex, noisy, and individual. Any technology that hopes to interface with it meaningfully must respect that complexity. The most exciting developments in neurotechnology aren’t just about better hardware or smarter algorithms. They’re about building tools that adapt to the messy, beautiful reality of human cognition—not the other way around.
So, should you discover the future of brain-computer interfaces today? Yes, but with eyes wide open. The future isn’t a single destination. It’s a series of careful, evidence-based steps. And the most valuable skill you can bring to that journey isn’t technical expertise. It’s patience, curiosity, and a willingness to separate genuine progress from well-meaning hype.
About the author: Asad Ansari is a dedicated Neurology Technician specializing in EEG and NCV at Amrita Hospital, Faridabad. Based in Delhi and a graduate of Jamia Millia Islamia, Asad brings hands-on expertise to neurodiagnostic procedures. He focuses on delivering precise, reliable data to neurologists while always prioritizing a comfortable and reassuring experience for his patients.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. BCIs, especially invasive implants, carry significant risks and should only be pursued under qualified medical supervision.



